Cosmetic Lower Limb Lengthening: Risks & Available Options
Medically Limb lengthening procedures are indicated when there is some obvious deformity or limb length
discrepancy. But compelled by the psychosocial implications of short stature for patients, Dr Gaurav Bhardwaj
and his team are increasingly dealing with distraction osteogenesis for cosmetic limb lengthening. To the
degree this is a realistic expectation. But evaluation of the risks and benefits of this treatment are very
important.
Limb lengthening with the Ilizarov / monorail apparatus has been used for pathological conditions such as
dwarfism, hemimelia and other congenital or acquired limb-length discrepancy years and in recent years we
have broadened the scope to include cosmetic and psychological indications based upon patient demand.
Under Dr Gaurav Bhardwaj team’s strict protocol the treatment typically starts with patient’s interview to take
him/her through the planned procedure and post operative course which is demanding both physically and
psychologically. The treatment generally involves first surgery where bone is cut ( corticitomy) at the selected
site, most common around the knee and 3-4 pins are put on both sides of the cut connected by a frame which
remains outside the skin ( therefore called as external fixator).. Frame comes with a distraction device. Within
few days of surgery, patient is taught to start gradual distraction which should be strictly followed. Gentle pulling
of bony cut ends apart ensures the bone remains sticky as it increases in length. Too slow bone will heal back
and won’t increase in height, too fast the ends will go away with no stickiness between meaning a fracture
which won’t unite. Nowadays some doctors also put a nail in the bony canal to maintain the bony alignment.
It is safe to increase height by 5-6 centimeters, as the nerves, muscles and vessels may not tolerate more than
this. During this process which is dynamic there may be loss of alignment, deformity developement, pin
infection or loosening or several other reasons needing additional interventions. Once required gain in height is
achieved frame is kept on for around 2 more months for bone to get consolidated. If frame is removed too soon
the bone can recoil back and height gain is lost. Once bone has healed fixator and pins need to be removed.
The indications for surgery are (1) the presence of a clear reason to undergo limb lengthening, (2) strong
motivation, and (3) consented to undergo the procedure after complete awareness of the nature of surgery,
possible complications, and the rehabilitation program.
On the basis of the established criteria, treatment outcome is excellent in ~55% patients, good in ~40%.
Risks of pin tract and soft tissue infections, neuropathy ( stretching of the nerve causing sensory or movement
dysfunction), and joint displacements. Regular assessment of hip. knee and ankle ROM during and after
external fixation to assess for soft tissue complications and clinic-radiologic monitoring for hip, knee and ankle
congruity are done to rule out any sub-luxations. There may be incidences of osteomyelitis during treatment.
When distraction is commenced which is painstaking procedure, speed of regeneration, incidence of any
deformity, or fracture of regenerate during and after external fixation should be closely monitored for.
Living with fixators and pins poking out of legs for months, keeping pin sites clean to prevent them from getting
infected and need to follow the rigorous compliance with distraction and non weight bearing needs very strong
will power and motivation.
Soft tissue complications (~28%) of which (46%) may need re-interventions.
1. Pin tract infections (~3.82%),
2. Neuropathy (~ 4.58%),
3. Equinus of the ankle (~9.16%),
4. Fixed flexion deformity of the knee (~ 11%).
Bone-related complications ~17% of which (~73%) needed re-interventions.
1. Incomplete corticotomy of the tibia that needed osteoclasis
2. Premature fibular consolidation requiring reosteotomy with the patient under anesthesia
3. Osteomyelitis ( deep bone infection)
4. Delayed regeneration / non union
5. Deformity of the regenerate while wearing the fixator,
6. Deformity of the regenerate after removal of the fixator
7. Subluxation of joint.
8. Late fracture through the regenerated bone.
In conclusion the decision to undergo both limb lengthening by bone distraction for cosmetic increase in height
is a serious decision. It should be taken only after fully understanding the complexities of the surgical
procedures, possible complications, psychological dimensions and with realistic expectations.
discrepancy. But compelled by the psychosocial implications of short stature for patients, Dr Gaurav Bhardwaj
and his team are increasingly dealing with distraction osteogenesis for cosmetic limb lengthening. To the
degree this is a realistic expectation. But evaluation of the risks and benefits of this treatment are very
important.
Limb lengthening with the Ilizarov / monorail apparatus has been used for pathological conditions such as
dwarfism, hemimelia and other congenital or acquired limb-length discrepancy years and in recent years we
have broadened the scope to include cosmetic and psychological indications based upon patient demand.
Under Dr Gaurav Bhardwaj team’s strict protocol the treatment typically starts with patient’s interview to take
him/her through the planned procedure and post operative course which is demanding both physically and
psychologically. The treatment generally involves first surgery where bone is cut ( corticitomy) at the selected
site, most common around the knee and 3-4 pins are put on both sides of the cut connected by a frame which
remains outside the skin ( therefore called as external fixator).. Frame comes with a distraction device. Within
few days of surgery, patient is taught to start gradual distraction which should be strictly followed. Gentle pulling
of bony cut ends apart ensures the bone remains sticky as it increases in length. Too slow bone will heal back
and won’t increase in height, too fast the ends will go away with no stickiness between meaning a fracture
which won’t unite. Nowadays some doctors also put a nail in the bony canal to maintain the bony alignment.
It is safe to increase height by 5-6 centimeters, as the nerves, muscles and vessels may not tolerate more than
this. During this process which is dynamic there may be loss of alignment, deformity developement, pin
infection or loosening or several other reasons needing additional interventions. Once required gain in height is
achieved frame is kept on for around 2 more months for bone to get consolidated. If frame is removed too soon
the bone can recoil back and height gain is lost. Once bone has healed fixator and pins need to be removed.
The indications for surgery are (1) the presence of a clear reason to undergo limb lengthening, (2) strong
motivation, and (3) consented to undergo the procedure after complete awareness of the nature of surgery,
possible complications, and the rehabilitation program.
On the basis of the established criteria, treatment outcome is excellent in ~55% patients, good in ~40%.
Risks of pin tract and soft tissue infections, neuropathy ( stretching of the nerve causing sensory or movement
dysfunction), and joint displacements. Regular assessment of hip. knee and ankle ROM during and after
external fixation to assess for soft tissue complications and clinic-radiologic monitoring for hip, knee and ankle
congruity are done to rule out any sub-luxations. There may be incidences of osteomyelitis during treatment.
When distraction is commenced which is painstaking procedure, speed of regeneration, incidence of any
deformity, or fracture of regenerate during and after external fixation should be closely monitored for.
Living with fixators and pins poking out of legs for months, keeping pin sites clean to prevent them from getting
infected and need to follow the rigorous compliance with distraction and non weight bearing needs very strong
will power and motivation.
Soft tissue complications (~28%) of which (46%) may need re-interventions.
1. Pin tract infections (~3.82%),
2. Neuropathy (~ 4.58%),
3. Equinus of the ankle (~9.16%),
4. Fixed flexion deformity of the knee (~ 11%).
Bone-related complications ~17% of which (~73%) needed re-interventions.
1. Incomplete corticotomy of the tibia that needed osteoclasis
2. Premature fibular consolidation requiring reosteotomy with the patient under anesthesia
3. Osteomyelitis ( deep bone infection)
4. Delayed regeneration / non union
5. Deformity of the regenerate while wearing the fixator,
6. Deformity of the regenerate after removal of the fixator
7. Subluxation of joint.
8. Late fracture through the regenerated bone.
In conclusion the decision to undergo both limb lengthening by bone distraction for cosmetic increase in height
is a serious decision. It should be taken only after fully understanding the complexities of the surgical
procedures, possible complications, psychological dimensions and with realistic expectations.
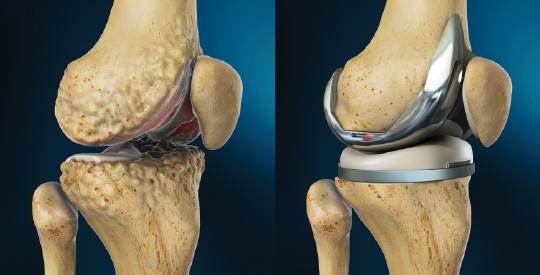
Knee implants prices capped- benefit to patients
An interesting news in today newspapers about government of india through National Pharmaceuticals Pricing Authority capping the prices of knee implants. As had been done in cases of cardiac stents there had been reports of profiteering in the implants and panel had been working to streamline the process. Since last evening, when this news came in I received numerous calls from orthopaedic colleagues and patients about likely impact of this announcement.
By reducing the cost of the implants, the treatment of painful arthritis will be cheaper and affordable. It should encourage people to go ahead and get rid of their painful arthritic knees which they were carrying on for long. Health services have to be affordable and in universal reach for them to be meaningful.
As a knee surgeon, I am very happy for my patient as cost should come down. It should also instill trust in medical care as the fear of profiteering in the medical implants is being eliminated. This will help in restoring the patient doctor relationship of trust, which is under severe strain nowadays. Patient will feel reassured they are not fleeced on knee replacement implant costing.
But as had been seen in cases of cardiac stent I donot want new prices to be deterrent for Impalnt companies to bring their latest implants in Indian markets. We cannot be in a situation where we are deprived of the best of the implants as company finds them economically unviable. For that the prices which are fixed yesterday will be reviewed periodically and a robust mechanism should be there to ensure our patients are not denied world class quality implants.
To conclude this is a very positive step, with the noble intention of keeping patients well being supreme. But this is not one time action and a constant review is important to keep pace with time and ever changing medical technology.
By reducing the cost of the implants, the treatment of painful arthritis will be cheaper and affordable. It should encourage people to go ahead and get rid of their painful arthritic knees which they were carrying on for long. Health services have to be affordable and in universal reach for them to be meaningful.
As a knee surgeon, I am very happy for my patient as cost should come down. It should also instill trust in medical care as the fear of profiteering in the medical implants is being eliminated. This will help in restoring the patient doctor relationship of trust, which is under severe strain nowadays. Patient will feel reassured they are not fleeced on knee replacement implant costing.
But as had been seen in cases of cardiac stent I donot want new prices to be deterrent for Impalnt companies to bring their latest implants in Indian markets. We cannot be in a situation where we are deprived of the best of the implants as company finds them economically unviable. For that the prices which are fixed yesterday will be reviewed periodically and a robust mechanism should be there to ensure our patients are not denied world class quality implants.
To conclude this is a very positive step, with the noble intention of keeping patients well being supreme. But this is not one time action and a constant review is important to keep pace with time and ever changing medical technology.
Whole body pains- it can be fibromyalgia
Mrs X, looking very worried walked into my OPD chamber with her very concerned family. She has not been keeping well for last few months. Her main problem is having wide spread joints and muscles pain all over her body. She is troubled by sleep disturbance

Do not give up sports training in blistering summer- safety tips
While many of us spend day staying away from sweltering sun as much as possible there are some of us specially athletes who sweat it out on fields to make us proud.
Though continuous
Though continuous
Clotting in leg going into lungs can be deadly
The incidence of spontaneous developement of clot formation in leg muscles called as Deep Vein Thrombosis (DVT) and then migrating to lungs is called as Pulmonary Embolism (PE), is not uncommon and stands out as 1 in 1000. Though anyone can develope this condition there are certain risk factors associated. The risk factors are immobility caused by trauma, surgery, increasing age or even prolonged journey, obesity, pregnancy, cancer or hormones like oral contraceptives. Thrombosis can be potentially fatal. PE is said to be cause in up to 30% of sudden unexplained deaths.
This condition can present either as swelling and pain in the muscles of the legs. The diagnosis at this stage isn't doppler scan or rarely angiography. In case of thrombosis going into lungs a person can feel breathless or get collapsed. The diagnosis in this case is by CT angio.
Thrombosis is generally caused due to stagnation of blood in the leg muscles causing clots or when blood clots abnormally. So one has to prevent prolonged immobilisation like sitting in flight over long periods. More than 4 hours of journey doubles the risk of thrombosis, also called as economic travel syndrome though it can also happen in car or train journey.
So the prophylaxis for this condition in journey is having regular walks and stretches along with keeping self well hydrated by drinking lots of water and avoiding alcoholic drinks.
As this condition mainly affects after surgery it is very important to start early mobilisation to prevent thrombosis. Now a days patient specially those with cancer or with fractures or undergoing joint replacements in hospital are put on calf pumps to prevent clotting of the blood in leg muscles while they are in the bed. More and more techniques are used which ensure early mobilisation of the patients. Doctors also prescribe blood thinner swherever needed to prevent same. The treatment with blood thinners is generally given under close watch.
One should be very particular about checking on a hospitalised patient if thrombosis prevention is being implemented. A good understanding and avoiding the risk factors for this potentially fatal condition can go long way in improving the clinical outcomes.
What are generic & branded medicines
Generic medicines are those which are sold by the names of the actual medicine salt they contain( the one which you see in the ingredient lists of the tablet strip or syrup bottle).
The concern had been that big pharma companies manufacturing these under their brand name make huge profits. There are expectation, by letting patient buy generic rather than brand, a better price will be ensured . But will this actually happen in today's situation? Will quality be ensured? The plain and simple honest answer is NO.
Why??
Let's start will a simple scenario. You buy a soap by asking for a "soap" or you trust a company brand name. The answer is we shortlist one company name after deciding about its quality and authenticity by media or personal experience. So can we leave all important decision of buying medicines on shopkeeper, in this case chemists?
There is widespread doubt that doctors write medicine with some motive. The answer is yes, there is a motive behind. As an expert professional, doctors go through the research and manufacturing standards of that medicine. They study various scientific studies and patient outcomes. They discuss their clinical experience in the peer groups. They write a prescription with a simple motive of providing a good quality medicine as they are held responsible for clinical outcome. They donot act as brand ambassadors for that product like people endorsing a product brand in TVs after taking a hefty fees (which people donot mind). Tell me what motivates s a famous actor to endorse a product ? Fees or a scientific study of that product but we donot crib about that and happily follow their endorsement.
Problem is if a doctor writes a generic name of Medicine, in present situation it will shift the privilege of deciding which medicines patient will be getting, to chemists. Now what is guarantee that chemist decision will not be influenced by profit margins. There are almost no generic available in Indian markets and when we say generic is actually a brand generic!!
Confused !! Rightly so.
So if a doctor writes a generic name, then chemist will decide which brand he or she will be dispensing. So decision will shift from doctor to chemist. Is it a comfortable thought?
That's why the doctors association are asking government, first to take out all loopholes so that patient get generic medicine with cost benefit without compromising on quality. So all branded should be gradually phased out and all medicines with same constituents will be available on same price for all manufactures following same quality standards. This will be like a situation where buying milk there will be only MILK written ( Not Amul, mother dairy or any other brand) as prices and standards will be same. Till then let's donot do anything in haste which can badly backfire.
Let's start trusting doctors.
The concern had been that big pharma companies manufacturing these under their brand name make huge profits. There are expectation, by letting patient buy generic rather than brand, a better price will be ensured . But will this actually happen in today's situation? Will quality be ensured? The plain and simple honest answer is NO.
Why??
Let's start will a simple scenario. You buy a soap by asking for a "soap" or you trust a company brand name. The answer is we shortlist one company name after deciding about its quality and authenticity by media or personal experience. So can we leave all important decision of buying medicines on shopkeeper, in this case chemists?
There is widespread doubt that doctors write medicine with some motive. The answer is yes, there is a motive behind. As an expert professional, doctors go through the research and manufacturing standards of that medicine. They study various scientific studies and patient outcomes. They discuss their clinical experience in the peer groups. They write a prescription with a simple motive of providing a good quality medicine as they are held responsible for clinical outcome. They donot act as brand ambassadors for that product like people endorsing a product brand in TVs after taking a hefty fees (which people donot mind). Tell me what motivates s a famous actor to endorse a product ? Fees or a scientific study of that product but we donot crib about that and happily follow their endorsement.
Problem is if a doctor writes a generic name of Medicine, in present situation it will shift the privilege of deciding which medicines patient will be getting, to chemists. Now what is guarantee that chemist decision will not be influenced by profit margins. There are almost no generic available in Indian markets and when we say generic is actually a brand generic!!
Confused !! Rightly so.
So if a doctor writes a generic name, then chemist will decide which brand he or she will be dispensing. So decision will shift from doctor to chemist. Is it a comfortable thought?
That's why the doctors association are asking government, first to take out all loopholes so that patient get generic medicine with cost benefit without compromising on quality. So all branded should be gradually phased out and all medicines with same constituents will be available on same price for all manufactures following same quality standards. This will be like a situation where buying milk there will be only MILK written ( Not Amul, mother dairy or any other brand) as prices and standards will be same. Till then let's donot do anything in haste which can badly backfire.
Let's start trusting doctors.
Trouble returns to delhi
Today woke up again to read the threat of dengue and Chinky returning this year. Last year I saw so many patient who were crying in pain and debilitated by these diseases. Prevention is most important followed by seeking medical help timely. Stay safe. Wish civic agencies get their act together and citizens donot have to suffer.
Total Knee Replacement – The Latest Trends
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam.

Myths About Joint Replacement
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam.

Sports Injuries
Lorem ipsum dolor sit amet, consectetur adipiscing elit, sed do eiusmod tempor incididunt ut labore et dolore magna aliqua. Ut enim ad minim veniam.